Return to flip book view
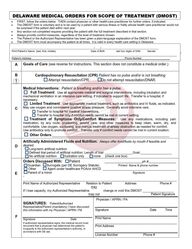
DELAWARE MEDICAL ORDERS FOR SCOPE OF TREATMENT (DMOST) • FIRST, follow the orders below. THEN contact physician or other health-care practitioner for further orders, if indicated. • The DMOST form is voluntary and is to be used by a patient with serious illness or frailty whose health care practitioner would not be surprised if the patient died within next year. • Any section not completed requires providing the patient with the full treatment described in that section. • Always provide comfort measures, regardless of the level of treatment chosen. • The Patient or the Authorized Representative has been given a plain-language explanation of the DMOST form. • The DMOST form must accompany the patient at all times. It is valid in every health care setting in Delaware. A Goals of Care (see reverse for instructions. This section does not constitute a medical order.) B Cardiopulmonary Resuscitation (CPR) Patient has no pulse and/or is not breathing Attempt resuscitation/CPR. Do not attempt resuscitation/DNAR. C Medical Interventions: Patient is breathing and/or has a pulse. Full Treatment: Use all appropriate medical and surgical interventions, including intubation and mechanical ventilation in an intensive care setting, if indicated to support life. Transfer to a hospital, if necessary. Limited Treatment: Use appropriate medical treatment, such as antibiotics and IV fluids, as indicated. May use oxygen and noninvasive positive airway pressure. Generally avoid intensive care. Transfer to hospital for medical interventions. Transfer to hospital only if comfort needs cannot be met in current setting. Treatment of Symptoms Only/Comfort Measures: Use any medications, including pain medication, by any route, positioning, wound care, and other measures to keep clean, warm, dry, and comfortable. Use oxygen, suctioning, and manual treatment of airway obstruction as needed for comfort. Use antibiotics only to promote comfort. Transfer only if comfort needs cannot be met in current location. Other Orders:_____________________________________________________________ D Artificially Administered Fluids and Nutrition: Always offer food/fluids by mouth if feasible and desired. Long-term artificial nutrition Defined trial period of artificial nutrition: Length of trial: ________________Goal:__________________ No artificial nutrition hydration only none (check one box) E Orders Discussed With: Patient ______________________ph.#________________ Guardian Surrogate (per DE Surrogacy Statute) Printed Name & phone number Other Agent under healthcare POA/or AHCD __________________________________________ Parent of a minor Signature -________________________________________________________________________________________Print Name of Authorized Representative Relation to Patient Address Phone # may If I lose capacity, my Authorized Representative change or void this DMOST __________________ may not Patient Signature F SIGNATURES: Patient/Authorized Representative/Parent (mandatory) I have discussed this information with my Physician / APRN / PA Signature Date If authorized representative signs, the medical record must document that a physician has determined the patient’s incapacity & the authorized representative’s authority, in accordance with DE law. Physician / APRN / PA Signature Date Time Print Name _______________________________________ Print Address License Number Phone # ___________________________________________________________/____/_________________________________________ Print Patient’s Name (last, first, middle) Date of Birth last four digits of SSN Gender _______________________________________________________________ _________________________________________ Patient’s Address Phone Number
COMPLETING A DMOST FORM • Must be signed by a Licensed Physician, Advance Practice Registered Nurse, or Physician’s Assistant.• Use of original form is highly encouraged. Photocopies and faxes of signed DMOST forms are legal and valid.• Any incomplete section of a DMOST form indicates the patient should get the full treatment described in that section.REVIEWING A DMOST FORM -- It is recommended that a DMOST form be reviewed periodically, especially when: • The patient is transferred from one care setting or care level to another,• There is a substantial change in the patient’s health status, or• The patient’s treatment preferences change.MODIFYING AND VOIDING INFORMATION ON A COMPLETED DMOST FORM A patient with decision-making capacity can void a DMOST form at any time in any manner that indicates an intent to void. Any modification to the form voids the DMOST form. A new DMOST form may be completed with a health care practitioner. Forms are available online at www.delaware.gov/. SECTION A This section outlines the specific goals that the patient is trying to achieve by this treatment plan. Health care professionals shall share information regarding prognosis with the patient in order to assist the patient in setting achievable goals. Examples may include: • Longevity, cure, remission or better quality of life• To live long enough to attend an important event (wedding, birthday, graduation)• To live without pain, nausea, shortness of breath or other symptoms• Eating, driving, gardening, enjoying time with family, or other activitiesSECTION B This is a medical order. Mark a selection for the patient’s preferences regarding CPR. SECTION C This is a medical order. When “limited treatment” is selected, also indicate whether the patient prefers or does not prefer transfer to a hospital for additional care. • IV medication to enhance comfort may be appropriate treatment for a patient who has indicated “symptom treatmentonly.” • Non-invasive positive airway pressure includes continuous positive airway pressure (CPAP) and bi-level positiveairway pressure (Bi-PAP). • The patient will always be provided with comfort measures.• Patients who are already receiving long-term mechanical ventilation may indicate treatment limitations on the“Other Orders” line.SECTION D This is medical order. Mark a selection for the patient’s preferences regarding nutrition and hydration. Check one box. • Oral fluids and nutrition should always be offered if feasible and consistent with the goals of care.SECTION E This section documents with whom the medical orders were discussed, the name of any healthcare professional who assisted in the completion of the Form, the name of any authorized representative and if the authorized representative may not modify/void the Form. SECTION F To be valid, all information in this section must be completed. HIPAA PERMITS DISCLOSURE OF DMOST FORMS TO OTHER HEALTH CARE PROFESSIONALS AS NECESSARY FOR TREATMENT. SEND FORM WITH PATIENT WHENEVER MOVED TO A NEW SETTING Faxed, Copied, or Electronic Versions of the Form are legal and valid. DIRECTIONS FOR HEALTH-CARE PROFESSIONALS
Delaware Medical Orders for Scope of Treatment (DMOST) DMOST is a process for documenting treatment choices. The DMOST form is voluntary. It is a portable, standardized Medical Order that will be recognized and followed by Delaware health care providers. The DMOST conversation is an opportunity to understand the likely course of your health and medical condition, so that you may make informed choices that are appropriate and reflect what you want. If you choose, you may invite loved ones to join this conversation. Q. What is DMOST? A. The Delaware Medical Orders for Scope of Treatment (DMOST) form is a portable medical order form. It allows you to make choices about life-sustaining treatments, including among other treatments, CPR (resuscitation) and artificial nutrition. You may request full treatment, limited treatment, or comfort care only. Q. Who is it for? A. A DMOST form can be used by a person with a serious illness or frailty, whose health-care practitioner would not be surprised if they died within the next year. Q. When should it be discussed and signed? Who signs it? A. A DMOST form is completed after a conversation you have with a health care practitioner. It is signed by you and a physician (MD or DO), an advanced practice registered nurse (APRN), or a physician assistant (PA). The physician/APRN/PA signature makes the choices into portable medical orders. Q. Who is required to follow the wishes documented on the DMOST form? A. These orders will be followed by health care providers in any setting (ambulance, long-term care facility, emergency room, hospital, hospice, home, assisted living facility, etc.). It travels with you and is honored when you move to a new setting. Q. Can someone else make DMOST decisions for me? A. You make health-care decisions for yourself as long as you have decision-making capacity. You have the right to change your authorized representative at any time while you have decision-making capacity. If a physician determines that a person lacks decision-making capacity, an authorized representative can sign a DMOST form on behalf of that person. A DMOST form does not change the decision-maker designated by an Advance Health Care Directive, a Health Care Power of Attorney document, a guardian of person appointed by a Court, or Delaware law on health care surrogates. If you have capacity and complete a DMOST form, you can sign on the form saying that if you lose capacity, your authorized representative cannot void the form you signed. Q. What if I change my mind? A. If your condition or your choices change, you or your authorized representative should void (cancel) your DMOST form and request a new DMOST be completed with your new choices. You can void a DMOST form if you change your mind but do not want to create a new one. You may not make any changes to the content of the DMOST form. If you want to change your DMOST form you must void your previous form and complete a new one with your health-care practitioner. If your DMOST form does not agree with your advance directive, the most recent document will be followed. Q. Must I do this? A. The DMOST form is always voluntary and can be voided at any time. A Health care organization is prohibited from requiring you to complete a DMOST form for any reason, including as part of a person’s admission to a health care facility. It is important to understand that this form contains medical orders. It will be followed by health care providers. For example, if you choose “Do Not Attempt Resuscitation”, and your heart stops, no attempt will be made to restart your heart. If you choose “Intubate/Use Artificial ventilation”, then you may be placed on a breathing machine with a tube in your throat and transferred to an intensive care setting in a hospital. Q. What will happen to my choices if I travel out of state? A. Many states, including all the states in our region, currently use a form similar to the DMOST form. Forms from those states which are valid under the Delaware Law will be honored in Delaware. DMOST forms will be honored in other states which have reciprocity.